An interactive guide to understanding and overcoming the persistent challenge of low reimbursement for unlisted Durable Medical Equipment (DME) codes.
The Reimbursement Divide
The core issue isn’t new; it’s systemic. Unlisted codes lack a pre-defined value, forcing them down a slow, manual, and subjective path that contrasts sharply with the automated processing of standard codes.
Standard Code Path (Automated)
- Claim Submitted with Specific Code
- Automated Adjudication System
- Payment based on Pre-set Fee Schedule
Unlisted Code Path (Manual)
- Claim Submitted with Unlisted Code
- Pends for Manual Review & Scrutiny
- Subjective “By Report” Pricing or Denial
A System Under Pressure
The challenge of unlisted codes is magnified by broader industry pressures, creating an unsustainable financial environment for DME providers.
- Over 42% of DME suppliers have closed their doors since 2013, citing unsustainable reimbursement pressures.
- Medicare DMEPOS rates have not received a market-based inflation adjustment since 2016.
- As of Jan 2024, top product categories saw average reimbursement cuts of 20.1% in non-rural areas.
Payer Policy Explorer
While the core problem is universal, specific policies and reimbursement tactics vary significantly by payer. Use the tabs below to explore their approaches.
Medicare’s Approach
Medicare’s pricing for unlisted DME is often based on historical data, not current costs. For many items, payment is derived from average reasonable charges from **1986/1987**, increased only by minimal update factors. This means reimbursement is fundamentally disconnected from modern manufacturing and operational costs.
- Lowest Level APC: Under the Outpatient Prospective Payment System (OPPS), unlisted codes are often assigned to the lowest-level Ambulatory Payment Classification, packaging the payment into other services.
- Outdated Baselines: Reliance on decades-old cost data leads to chronically low reimbursement rates for items billed under codes like E1399.
- Push for Granularity: CMS has acknowledged the issue, proposing more specific codes based on purchase price to allow for more accurate fee schedule pricing in the future.
Medicaid’s State-by-State Maze
Medicaid reimbursement is a “Wild West” scenario, with massive variations between states and managed care plans. Below are examples from the plans you’re seeing issues with.
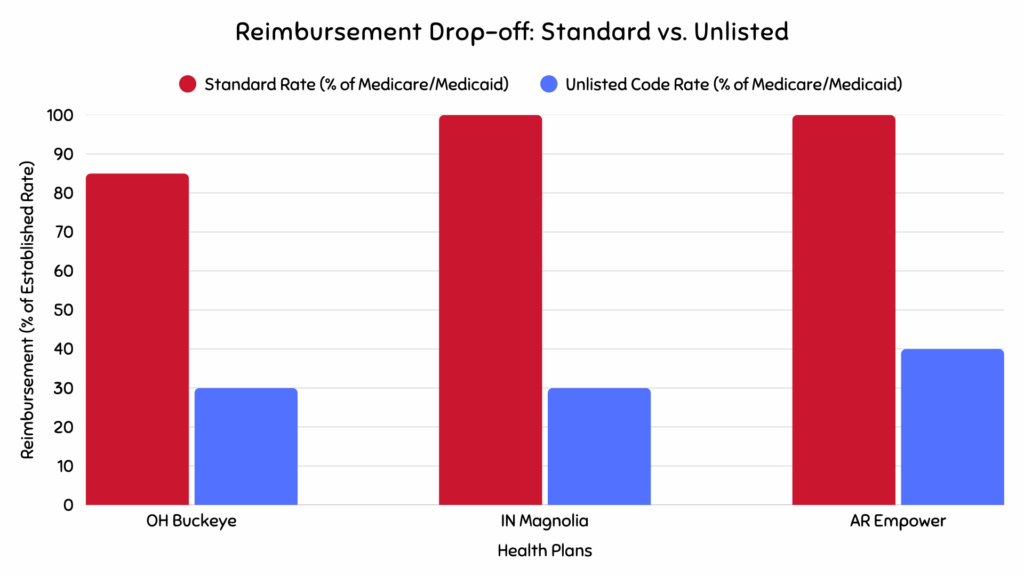
- Ohio Buckeye Health Plan: The “Lesser Cost” Mandate Buckeye’s policy denies higher-cost items if a “medically necessary, lesser-cost item” is deemed sufficient. This creates a reimbursement ceiling, forcing providers to accept payment at the rate of a cheaper alternative, even if the unlisted item offers superior outcomes.
- Indiana Magnolia Health Plan: The “Experimental” Hurdle Magnolia frequently denies unlisted items by classifying them as “experimental, investigational or unproven.” This places a huge burden on providers to prove that an innovative, unlisted item is widely accepted, a high bar for new technology.
- Arkansas Empower: The “Payment in Full” Trap Empower’s “payment in full” clause means providers are prohibited from balance billing patients. When combined with a low “by report” valuation, providers have no leverage and must accept the offered amount, shifting all financial risk onto them.
Commercial Payer Strategy
Commercial payers align with government programs but often use the administrative burden as a cost-containment tool. The “low reimbursement” is not just the dollar amount paid, but the profitability eroded by the immense effort required to get a claim approved.
- Universal Prior Authorization: This is a non-negotiable prerequisite. Failure to obtain it is the most common reason for denial.
- No Extra for Complexity: Policies often explicitly state that no additional reimbursement is given for special techniques or higher-cost equipment, even if justified.
- Documentation as a Barrier: Stringent and complex documentation requirements create a high administrative burden, discouraging providers or forcing them to accept low payments to avoid costly appeals.
Provider’s Action Plan
Maximizing reimbursement requires a proactive, multi-faceted strategy. Use this checklist to optimize your billing process for unlisted codes.
1. Proactive Payer Communication
Shift the burden of determination to the payer *before* service. This is a “pre-emptive strike” against denials.
- Always obtain Prior Authorization before rendering the service.
- Contact the payer directly to understand their specific policies and documentation requirements for the unlisted code in question.
- Confirm if a Category III code or specific modifier might be more appropriate.
2. Meticulous Documentation
Your documentation is your primary negotiation tool. Construct a compelling argument for your desired reimbursement.
- Detailed Narrative: Include item name, manufacturer, product number, and why it’s medically necessary.
- Clinical Support: Attach all relevant clinical notes (H&P, office notes, etc.), underlining the key supporting sections.
- Invoice: Always include a copy of the manufacturer’s invoice.
- Comparable Code Analysis: Propose a similar, valued code and explain how the unlisted item’s complexity compares (e.g., “50% more complex due to…”).
3. Effective Denial Management
A denial is a starting point, not an end point. A robust appeals process is essential for financial health.
- Understand common denial reasons: missing PA, insufficient documentation, “experimental” classification.
- Initiate a formal appeal promptly, adhering to the payer’s timely filing limits.
- Strengthen the appeal with additional clinical notes and resubmitted comparable code analysis.
- Conduct internal audits to prevent recoupments on paid claims, breaking the “denial-recoupment cycle.”
4. Industry Engagement
Individual providers have limited power. A collective voice can drive systemic change.
- Support industry advocacy groups working to improve reimbursement rates.
- Key organizations include the American Association for Homecare (AAHomecare) and the National Coalition for Assistive and Rehab Technology (NCART).
- Advocacy addresses root causes, like rate stagnation and competitive bidding, that individual billing strategies cannot solve.