Answer Summary:
Many DME providers believe that enrolling with “State Medicaid” (the government entity) automatically grants access to Medicaid Managed Care Organizations (MCOs) like “Aetna Better Health” or “UnitedHealthcare Community Plan.” This is false. Each MCO functions as a separate insurance company with its own credentialing application, contract cycle, and closed panels. Missing these separate enrollments means forfeiting access to 70%+ of the Medicaid volume in many states.
Introduction:
“I’m enrolled in Florida Medicaid, so I can see all Medicaid patients.”
Incorrect.
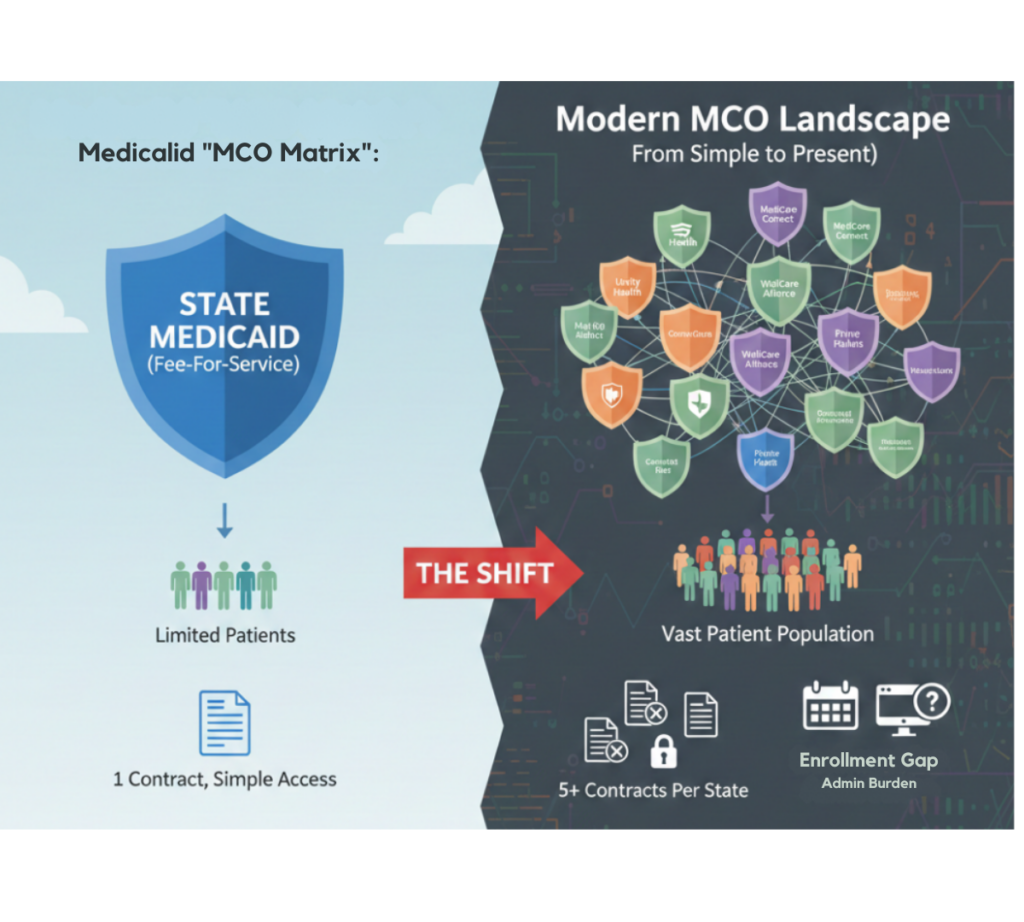
In 2026, most states have outsourced their Medicaid programs to private Managed Care Organizations (MCOs). If you are only enrolled with the state directly (Fee-For-Service), you are enrolled in a ghost town that covers fewer and fewer patients.
The real volume is in the MCOs. But getting into them is a contracting nightmare.
The “One State, Five Contracts” Problem
To cover a Medicaid patient in a state like Texas or Ohio, you don’t need one contract; you often need five.
- State Medicaid (The Foundation – Required for MCOs).
- MCO Plan A (e.g., Molina).
- MCO Plan B (e.g., AmeriHealth Caritas).
- MCO Plan C (e.g., Centene/Superior).
- The Pain: Each MCO has its own revalidation dates, its own portal (Availity, Syft, etc.), and its own “closed panel” rules.
The “Backdoor” Entry Strategy
MCO panels are notoriously difficult to crack. They often say “Network Closed.”
- The Strategy: Leverage your State enrollment.
- The Argument: Many states have “Continuity of Care” or “Any Willing Provider” clauses for Medicaid.
- The Play: If you are serving a patient under State Medicaid who gets auto-assigned to an MCO, the MCO is often required to offer you a “Single Case Agreement” (SCA) to keep the patient stable. Use this foothold to demand a full contract.
WWS Value Proposition:
We Manage the MCO Matrix
Contracting with 5 MCOs in 10 states equals 50 separate applications. Wonder Worth Solutions handles Medicaid MCO Credentialing at scale. We track the specific open/close dates for MCO panels and manage the roster submissions so you capture the full Medicaid population, not just the “Fee-for-Service” leftovers.
Are you missing 70% of Medicaid patients?
Let’s audit your MCO coverage for a Payer Coverage Analysis.