Answer Summary
“Mostly complete” applications are automatically rejected because payers treat missing Third-Party Administrator (TPA) or roster details as non-compliant, leading to a 35% failure rate that stalls revenue growth. Transitioning to digital submission portals with “hard gates” is the most effective strategy for meeting 2026 CMS interoperability and documentation standards while significantly reducing administrative rework. By enforcing data precision at the source, DME providers achieve a 35% higher success rate and faster in-network status.
The Scenario: The “Volume” Trap
“Summit Healthcare” was in the middle of an aggressive growth phase. The mandate from leadership was clear: expand the payer network as fast as possible to support new locations. The Provider Enrollment team responded by prioritizing volume. They churned out applications daily, focusing on getting them “out the door.”
On the surface, productivity looked high. But the outcome metrics told a different story. The team was running on a treadmill—moving fast but going nowhere. A deep-dive audit revealed that a staggering 35% of all applications were being rejected or closed by payers.
The Operational Failure
The root cause was not a lack of effort; it was a lack of precision. The primary reason for these rejections—accounting for 35% of the failure volume—was “Incomplete Documentation”
In their rush to meet submission targets, the team frequently skipped fields they deemed “optional” or “to be provided later.”
- The TPA Blind Spot: A specific recurring failure involved Third-Party Administrator (TPA) information. The team often failed to capture essential TPA details in the initial submission, assuming they could clarify it during negotiation.
- The Consequence: Payers do not view these fields as optional. To a payer, an application missing a TPA ID or a roster detail is not “pending”—it is “non-compliant.” These applications were often rejected outright or thrown into a low-priority queue, requiring weeks of back-and-forth emails to resurrect.
The WWS Solution: The Digital Submission Portal
To stop the bleeding, WWS moved the team from a manual, email-based submission process to a structured Digital Submission Portal. We replaced “guidelines” with “hard gates.”
1. Mandatory Field Logic
We configured the submission portal to act as a strict gatekeeper. We hard-coded logic that prevents the “Submit” button from functioning if key data points—specifically TPA details and NPI rosters—are missing. The system now forces the team to do the hard work of information gathering before the application leaves the building.
2. Payer-Specific Checklists
Recognizing that different payers have different “kill criteria,” we implemented payer-specific checklists. An application for UnitedHealthcare now triggers a different set of mandatory requirements than one for a regional TPA. This ensures that the application is tailored to the specific rejection triggers of that payer.
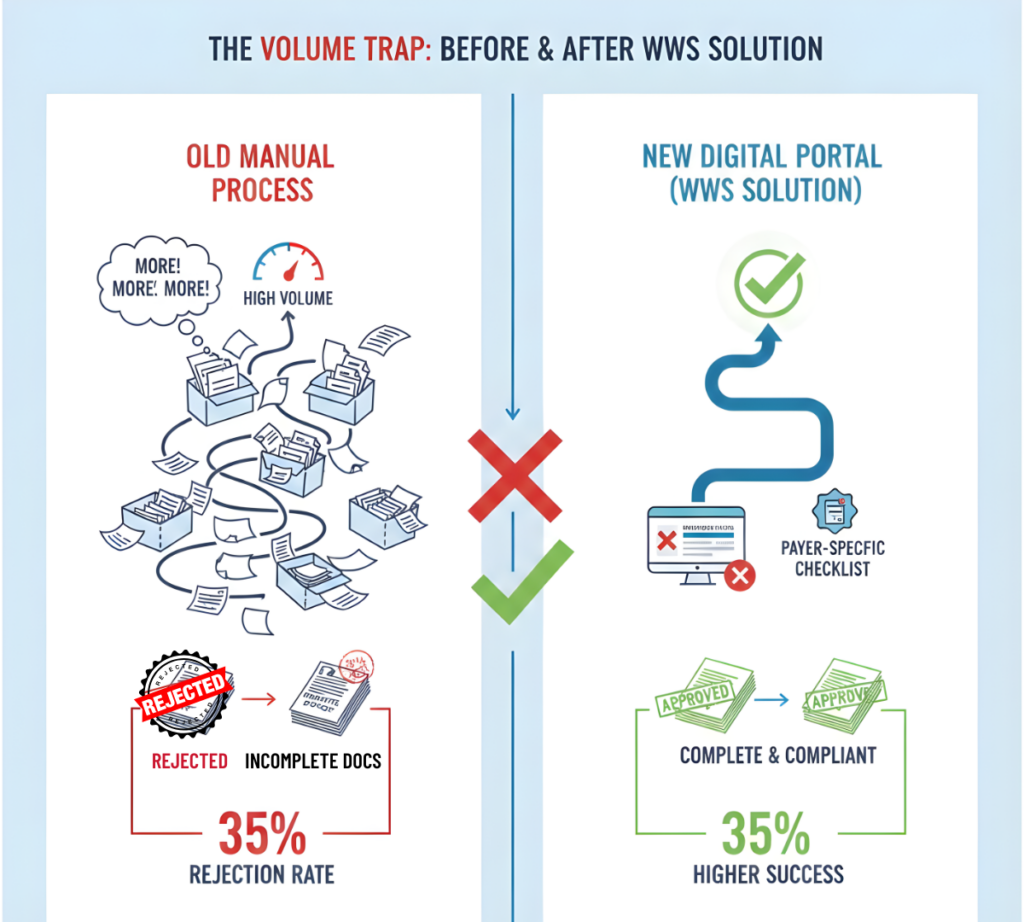
The Outcome
The impact of “getting it right the first time” was mathematically significant. Our analysis showed that applications with complete initial submissions demonstrated a 35% higher success rate than those requiring follow-up. By forcing compliance at the source, we transformed the team’s output from “High Volume/Low Quality” to “High Velocity/High Acceptance.”